The equine foot is an amazing structure.
It provides strength, stability and flexibility, all while representing an incredibly small amount of the entire equine mass. Yet, the foot is also the greatest source of all lameness. Any change to the foot can prove devastating for the horse.
“The design of the foot has evolved strategically to allow it to survive in a harsh environment with a high level of demand,” Mark Silverman told attendees at the September 2014 Northeast Association of Equine Practitioners Symposium in Norfolk, Va. “Alteration that occurs to the foot, whether through disease, injury, conformational irregularities or human intervention may have serious implications regarding the foot’s ability to cope with the rigors of day-to-day work.”
Silverman believes that it’s critical for farriers to understand the difference between physiological and pathological problems.
“Physiologic indicates conformation, structure, function and stress level that is within the normal or expected range for good health,” says Silverman, an equine veterinarian and farrier who partners with farrier Ernest Woodward at the Southern California Equine Podiatry Center in San Marco, Calif. “Along those same lines, pathologic indicates that one or more of these same features fall outside what is healthy
or sustainable.”
Outside the Norm
Although external marks often give farriers an indication of internal problems within the hoof capsule, complications can arise that don’t become readily apparent from
visual clues.
“It’s in these cases that we require additional input,” he says, “often in the form of radiographs, to better reveal the bony column’s alignment
and geometry.”
While other means of data collection — such as hoof testers, percussion, diagnostic blocks, MRI and nuclear scintigraphy — might be necessary, the clinical examination is the single most important tool for determining whether a problem is physiologic or pathologic.
“If we don’t recognize something as outside of normal,” Silverman says, “we won’t know to look further.”
Failing to correctly recognize a problem can lead to disastrous consequences for the horse.
“We will fall into the trap of addressing this troubled foot as a variation of normal,” he says, “and the underlying problem will continue to smolder, waiting for the day when it will become grossly obvious.”
Clinical Examination
Silverman was presented with a horse with a moderate club foot and rotational deformity (Figure 1). The clinical examination includes both static and dynamic observations, as well as radiographs.

Static observations. The hoof indicates a long bridge-to-toe and a short bridge-to-heel ratio (Figure 2). Compressed growth rings also are noted at the proximal portion of the dorsal wall.
“The first 2 cm of the dorsal wall are very steep, followed by a dorsal displacement of the wall as it progresses distally,” Silverman says. “The growth rings of the capsule are divergent at the heels and the heels themselves are unusually tall.”

The static examination also reveals a short, deep-set, atrophied frog in the palmar surface of the foot.
“The sole, cranial to the apex of the frog,” he says, “has no concavity and there is a distinctly bi-planar sole.”
Hoof testers also indicated sole sensitivity cranial to the apex of the frog (Figure 3).
Dynamic observations. The left front leg and the diagonal hind limb exhibit a short anterior phase during the stride. A pronounced heel-first landing pattern is also evident forthe forelimb.

“Also worth noting,” Silverman says, “is the rapid rotational acceleration of this foot at heel-off.”
Finally, the horse is experiencing an upward jamming of the shoulder, according to the rider.
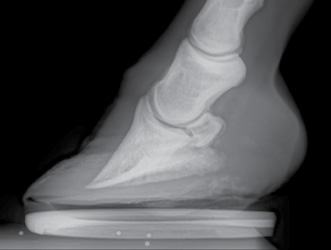
Radiographic observations. Examining the internal structures via a radiograph lends credence to the belief that the horse is club footed
(Figure 4).
“The palmar angle of the P3 is steep,” he says. “The horn-laminar zone (HLZ), measured at the top
portion of the dorsal wall and at the middle portion of the dorsal wall is equal, but there is an increase in the HLZ as you get to the distal portion of the dorsal wall.”
There also is some deformation of the coffin bone that causes concern.
“P3 is lipping at the distal margin of the dorsal portion of the bone, along with a curvilinear shape of the bone in general,” Silverman says. “The sole under this deformed section of P3 is only 10 mm thick. Mineralization of the collateral cartilages is quite advanced for a horse of this age
and experience.”
The 10-year-old horse has a history of soundness problems, so the hoof-care professionals have two choices.
“We know that we’re not going to simply make this a normal foot,” he says. “At this point, we can either fall into ‘shoeing the club foot mode,’ or we can think through the issues that this horse presents.”
Taking a Stepwise Approach
The clinical examination is successful in developing more information about the pathology of the foot.
“The horse has excess pressure on the cranial sole and tension trying to rotate P3 within the hoof capsule, which is displayed as hoof tester sensitivity and dorsal wall deformity,” Silverman determines. “The stress also has led to the compression of the dorsal growth rings, slowing hoof growth in the affected region.
“This foot wants to have less of a lever at the forward position of the hoof, acting against the effect of the deep digital flexor tendon (DDFT).”
The stepwise approach helps to formulate a more precise method for treating the details involved, rather than simply labeling the horse’s condition and treating for that condition.
“We may even need to trim this foot a bit more upright for a while to relax the DDFT until the stresses settle down,” he says. “Depending on the individual hoof, we may want to reshape the dorsal wall, eliminating some of the flare. A rolled or rockered toe might also be useful to smooth
the unrollment.”
The pronounced heel-first landing pattern, as well as the shoulder jamming, could be leading to additional shock at the caudal foot, Silverman says.
“Lowering the heel is not appropriate with what’s going on in the cranial portion of the foot,” he says, “but adding a caudal rocker, something more parallel to the base of P3 will help to smooth out the strike pattern of this foot.”
Success in a case such as this relies greatly upon cooperation between the farrier and the veterinarian.
“In the process, a long-term treatment plan for the horse will be established,” he says. “One added benefit of this protocol is that when the inevitable treatment failure occurs, the understanding achieved in each goal enables the farrier-vet team to fine tune it for improved results.”
Adaptive Shoeing Vs. Therapeutic Shoeing
Silverman stresses the importance of understanding the concept of adaptive shoeing and therapeutic shoeing when trying to understand the mechanics of the conditions that are being treated.
“This might seem a fine point and over thought,” he says, “but often we are treating conditions that are not going to heal.”
Many conditions that hoof-care professionals face day-in and day-out are permanent.
“Therapeutic shoeing implies that over time we will correct the condition,” Silverman explains. “Adaptive shoeing recognizes that we are working to accommodate an existing permanent condition. The person who lost a foot in an accident is not going to receive a therapeutic prosthesis. They will get an adaptive device to help them function well in day-to-day life.”
When a permanent condition is revealed, a farrier plays an increasingly critical role.
“We are not going to repair chronic low ringbone with a shoe,” he says. “Nor are we going to ameliorate chronic low-heel conformation, but we can optimize the shoeing of the individual to make the patient more comfortable and to minimize progressive damage to the foot.
“Wedging that low-heeled foot may provide temporary comfort, but over time the hoof capsule will become increasingly compromised.”
A Comprehensive Path
Silverman advocates a comprehensive approach that will benefit the horse for years to come.
“Address all of the factors of the condition to achieve the best overall result,” he says. “Is the patient’s low-heeled condition something that was created by us or does the horse have a tendon laxity issue that leads to an overloading of the hoof capsule?
“Attempting to determine the cause and history of a condition will be an aid in establishing a prognosis and a treatment plan.”
Addressing the individual factors in a case will often lead to a greater understanding. Thus, treatments are developed that otherwise might not have materialized.
“Since many diseases are poorly understood mechanically,” he says, “we often see therapeutic attempts that defy logic.”
Silverman encountered a young farrier who was caring for a horse with chronic, yet stable laminitis by using a heavy plastic pad in an effort to protect the frog from pressure.
“He understood that somehow the frog was involved in treating the disease,” he says. “He had not made the mechanical leap in understanding how.”
The heavy plastic pad might have been an adequate support technique, many farriers would have opted for some form of heart bar.
“The idea for this sort of a foot,” Silverman explains, “is to support the core structures and limit the challenge of the connection between the coffin bone and the hoof capsule.”
Although the young farrier involved the frog, he missed the mark on the purpose for its involvement.
“This farrier did something that might have provided some level of core support, but it was the wrong reason,” he says. “We are not trying to protect the frog from pressure, we are trying to utilize the frog to provide core support.
“While this may be an extreme example, there have been many cases in which a farrier who could fine-tune a show horse to perform at a
high level had failed to grasp the mechanical change that occurs in the laminitic foot.”
It Takes Teamwork
Silverman reiterates that the vet and farrier play critical roles in developing and implementing a treatment plan. Therefore, a good working relationship is absolutely crucial.
“The veterinarian will prove valuable in providing medical insight into the case, yet not appreciating a particular hoof capsule’s ability to tolerate a specific shoe or appliance will lead to potential treatment failure,” he says. “This is where the farrier’s expertise comes into play. It is often best to discuss the mechanical goal of the proposed treatment and then come to a consensus on the method to be used.”
The approach will be more time consuming, yet the results are worth it.
“By taking the time to appreciate the factors involved in a specific case, we can come up with a more comprehensive plan for treatment,” Silverman says. “As man has domesticated the horse and challenged it to perform new tasks, we have attempted to adapt the foot to help it endure
greater stress.
“The more that we strive to understand the function of the foot, the greater our chances of providing the needed modifications without compromising the evolutionary changes that have made the foot so thoroughly capable.”