American Farriers Journal
American Farriers Journal is the “hands-on” magazine for professional farriers, equine veterinarians and horse care product and service buyers.
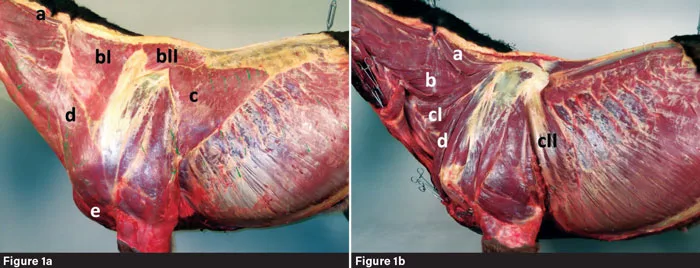
The components of the thoracic sling in Figure 1a are the (a) Rhomboideus, (bl) Trapezius cervicis, (bll) Trapezius thoracis, (c) Latissimus, (d) Brachiocephalicus and (e) Pectorales muscles. In Figure 1b, they are (a) Rhomboideus, (b) Omontransversarius, (cl) Serratus ventralis, (cll) Serratus ventralis thoracis and (d) Subclavius muscle. Photo by: Dr. Jenny Hagen
Several studies state that lameness is the most prevalent health problem in horses and the main reason for retirement from their leisure use or competitive life (Clegg 2011; Ely et al. 2009; Dyson 2001). In this context, most pathologies appear in the structures of the equine distal limb at the forelimbs.
Injuries and disorders of joints, tendons and ligaments occur frequently. In particular, degenerative bone diseases such as desmitis, osteoarthritis, osteoarthrosis and podotrochlosis are common diagnoses in the equine practice. Thereby, the occurrence of orthopedic disorders related to the distal limb is independent of the athletic level and use of horses. Elite, as well as non-elite, riding horses are affected by wear of the sensitive structures at the distal limb (Murray et al. 2010). The question is: Why are…

American Farriers Journal is the “hands-on” magazine for professional farriers, equine veterinarians and horse care product and service buyers.

American Farriers Journal is the “hands-on” magazine for professional farriers, equine veterinarians and horse care product and service buyers.
Download these helpful knowledge building tools

We are here to support you.
We stock a wide range of high-quality products from trusted brands to ensure durability, performance, and reliability in every job you undertake. Our extensive inventory of horseshoe products and farrier tools means you can find everything you need in one place, saving you time and effort. Your satisfaction is our top priority. We are committed to providing excellent customer service, prompt shipping, and hassle-free returns.